Obstetrics (from the Latin obstare, "to stand by") is the surgical specialty dealing with the care of a woman and her offspring during pregnancy, childbirth and the puerperium (the period shortly after birth). Midwifery is the equivalent non-surgical specialty. Most obstetricians are also gynaecologists. See Obstetrics and gynaecology.
The average gestational period for humans is 40 weeks by gestational age and 38 weeks by fertilization age. This is divided into three trimesters.
Veterinary obstetrics is the same concept for Veterinary medicine.
Antenatal care
In obstetric practice, an obstetrician or midwife sees a pregnant woman on a regular basis to check the progress of the pregnancy, to verify the absence of ex-novo disease, to monitor the state of preexisting disease and its possible effect on the ongoing pregnancy. A woman's schedule of antenatal appointment varies according to the presence of risk factors, such as diabetes, and local resources.
Some of the clinically and statistically more important risk factors that must be systematically excluded, especially in advancing pregnancy, are pre-eclampsia, abnormal placentation, abnormal fetal presentation and Intrauterine Growth Restriction.
For example, to identify pre-eclampsia, blood-pressure and albuminuria (level of urine protein) are checked at every opportunity.
Placenta praevia must be excluded (PP = low lying placenta that, at least partially, obstructs the birth canal and therefore warrants elective caesarean delivery); this can only be achieved with the use of an ultrasound scan. However, early placenta praevia is not alarming; this is because as the uterus grows along the pregnancy, the placenta may still move away. A placenta praevia is of clinical significance as from the 28th week of gestation. The current management includes a caeserrean section. The type of caeserrean section is determined by the position (anterior or posterior) of the placenta.In late pregnancy fetal presentation must be established: cepfalic presentation (head first) is the norm but the fetus may present feet-first or buttocks-first (breech), side-on (transverse), or at an angle (oblique presentation).
Intrauterine Growth Restriction is a general designation, where the fetus is smaller than expected when compared to its gestational age (in this case fetal growth parameters show a tendency to drop off from the 50th percentile eventually falling below the 10th percentile, when plotted on a fetal growth chart). Causes can be intrinsic (to the fetus) or extrinsic (maternal or placental problems).
Signs
Trimesters
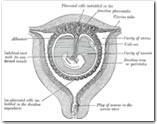
Anatomical model of a human pregnancy
First trimester: elevated β-hCG (human chorionic gonadotrophin) of up to 100,000 mIU/mL by 10 weeks GA is thought to contribute to morning sickness, fatigue, mood swings and food cravings. The symptoms can last through 12 to 16 weeks of gestation.
Second trimester: The abdomen shows an obvious swelling arising from the pelvis, starting the "obvious phase" of pregnancy. Hyperpigmentation, including linea nigra, may appear.
Third trimester: The mother may experience backaches due to increased strain. Typically, the curvature of the spine is changed as pregnancy evolves in order to counteract the change in weight distribution. The mother may also suffer mild urinary incontinence due to pressure on the bladder by the pregnant uterus, as well as heartburn(due to compression of the stomach).
Overall
»
Bluish discoloration of vagina and cervix (Chadwick's sign)
»
Softening and cyanosis of cervix after 4 weeks (Goodell's sign)
»
Softening of uterus after 6 weeks (Hegar's or Ladin's sign)
»
Breast swelling and tenderness
»
Linea nigra from umbilicus to pubis
»
Telangiectasias
»
Palmar erythema
»
Amenorrhea
»
Nausea and vomiting
»
Breast pain
»
Fetal movement
»
Sciatica (Pain caused by compression of the sciatic nerve)
Obstetrics
What is laparoscopic hysterectomy?
It is a procedure by which the uterus is removed laparoscopically. This is done with the aid of a telescope and very fine instruments, without making a big incision in the abdomen.
What are the advantages of laparoscopic hysterectomy?
The advantages over the conventional hysterectomy are that there is minimal tissue handling resulting in much less pain and lesser chances of adhesion formation after the operation. 2-3 very small incisions of 0.5-1.0 cm (as compared to 10-15cms in conventional procedure) are given on the abdomen resulting in less blood loss and lesser chances of wound infection with decreased hospital stay and early recovery as compared to conventional surgery.
Who can undergo laparoscopic hysterectomy?
Usually all the patients who have been advised for conventional hysterectomy can undergo laparoscopic hysterectomy, provided the size of uterus is not very big (that is bigger than 20 cm).
A person with diabetes or hypertension can also undergo this procedure after the conditions are under control, and in fact the advantages of lesser chances of infection and early recovery are very beneficial for them.
A patient who has undergone operations in the past can also undergo this procedure and if there are adhesions because of previous operations, they can be removed along with the laparoscopic hysterectomy, in the same sitting.
It is also possible to treat or remove the ovaries and tubes while carrying out laparoscopic hysterectomy.
What preparation is needed before the procedure?
The usual routine tests are required as for any other operative procedure and no special investigation is required for laparoscopic hysterectomy.
To make the operation easier, the recovery after the operation faster and resumption of normal work or activity earlier, some medicines along with diet restriction is started 2-3 days before the operation.
If the patient is fully investigated and has undergone an anaesthetic check up, she can get admitted on the morning of the operation.
How is the surgery performed?
This procedure is carried out under general anaesthesia. A small incision (about 1 cm) is made at the lower end of the navel. Through this a laparoscope is introduced inside the abdomen. It is a tube having lenses inside and a special camera attached to the outside end. This is then connected to a television monitor and allows the surgeon to see everything inside. After that two small half to one cm incisions are made on either side of the abdomen, to allow the introduction of thin long instruments, with which the operation is carried out.
What happens after the procedure?
The total hospital stay is usually for two days, after which one can go back home.
On an average, two hours after lunch and eight hours rest after dinner is what is usually recommended. The patient can climb stairs slowly, walk half to one km slowly and carry out sedentary work at home without much difficulty. One can bathe as the stitch dressing is usually waterproof.
Routinely, the patient is called seven days after the operation for the removal of stitches and then after six weeks for an internal check up.
When can one resume normal activity or go back to work?
Once the stitches are removed, the patient can resume normal activity like walking, jogging, cooking, driving, sitting in front of the computers for 4-6 hrs etc. Sexual intercourse, strenuous exercise, lifting of heavy weights and swimming. has to be avoided for six weeks.
Ovarian cyst
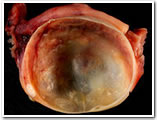
An ovarian cyst is any collection of fluid, surrounded by a very thin wall, within an ovary. Any ovarian follicle that is larger than about two centimeters is termed an ovarian cyst. An ovarian cyst can be as small as a pea, or larger than a cantaloupe.
Most ovarian cysts are functional in nature, and harmless (benign).[1] In the US, ovarian cysts are found in nearly all premenopausal women, and in up to 14.8% of postmenopausal women. The incidence of ovarian carcinoma is approximately 15 cases per 100,000 women per year.
Ovarian cysts affect women of all ages. They occur most often, however, during a woman's childbearing years.
Some ovarian cysts cause problems, such as bleeding and pain. Surgery may be required to remove those cysts.
Functional cysts
Some, called functional cysts, or simple cysts, are part of the normal process of menstruation. They have nothing to do with disease, and can be treated. There are 3 types, Graafian, Luteal, and Hemorrhagic.
Graafian follicle cyst
One type of simple cyst, which is the most common type of ovarian cyst, is the graafian follicle cyst, follicular cyst, or dentigerous cyst. This type can form when ovulation doesn't occur, and a follicle doesn't rupture or release its egg but instead grows until it becomes a cyst, or when a mature follicle involutes (collapses on itself). It usually forms during ovulation, and can grow to about 2.3 inches in diameter. It is thin-walled, lined by one or more layers of granulosa cell, and filled with clear fluid. Its rupture can create sharp, severe pain on the side of the ovary on which the cyst appears. This sharp pain (sometimes called mittelschmerz) occurs in the middle of the menstrual cycle, during ovulation. About a fourth of women with this type of cyst experience pain. Usually, these cysts produce no symptoms and disappear by themselves within a few months. Ultrasound is the primary tool used to document the follicular cyst. A pelvic exam will also aid in the diagnosis if the cyst is large enough to be seen. A doctor monitors these to make sure they disappear, and looks at treatment options if they do not.
Corpus luteum cyst
Another is a corpus luteum cyst (which may rupture about the time of menstruation, and take up to three months to disappear entirely). This type of functional cyst occurs after an egg has been released from a follicle. The follicle then becomes a secretory gland that is known as the corpus luteum. The ruptured follicle begins producing large quantities of estrogen and progesterone in preparation for conception. If a pregnancy doesn't occur, the corpus luteum usually breaks down and disappears. It may, however, fill with fluid or blood, causing the corpus luteum to expand into a cyst, and stay on the ovary. Usually, this cyst is on only one side, and does not produce any symptoms.
It can however grow to almost 4 inches in diameter and has the potential to bleed into itself or twist the ovary, causing pelvic or abdominal pain. If it fills with blood, the cyst may rupture, causing internal bleeding and sudden, sharp pain. The fertility drug clomiphene citrate (Clomid, Serophene), used to induce ovulation, increases the risk of a corpus luteum cyst developing after ovulation. These cysts don't prevent or threaten a resulting pregnancy.[13][14] Women on birth control pills usually do not form these cysts; in fact, preventing these cysts is one way the pill works.
Hemorrhagic cyst
A third type of functional cyst, which is common, is a Hemorrhagic cyst, which is also called a blood cyst, hematocele, and hematocyst.[16] It occurs when a very small blood vessel in the wall of the cyst breaks, and the blood enters the cyst. Abdominal pain on one side of the body, often the right side, may be present. The bleeding may occur quickly, and rapidly stretch the covering of the ovary, causing pain. As the blood collects within the ovary, clots form which can be seen on a sonogram.[17] Occasionally hemorrhagic cysts can rupture, with blood entering the abdominal cavity. No blood is seen out of the vagina. If a cyst ruptures, it is usually very painful. Hemorrhagic cysts that rupture are less common. Most hemorrhagic cysts are self-limiting; some need surgical intervention. Even if a hemorrhagic cyst ruptures, in many cases it resolves without surgery. Patients who don't require surgery will experience pain for 4 - 10 days after, and may require several days rest. Studies have found that women on tetracycline antibiotics recover 25% earlier than the majority of patients, a surprising correlation found in 2004. Sometimes surgery is necessary,[18] such as a laparoscopy ("belly-button surgery" that uses small tools inserted through one or more tiny slits in the abdomen).
Endometrioid cyst
An endometrioma, endometrioid cyst, endometrial cyst, or chocolate cyst is caused by endometriosis, and formed when a tiny patch of endometrial tissue (the mucous membrane that makes up the inner layer of the uterine wall) bleeds, sloughs off, becomes transplanted, and grows and enlarges inside the ovaries. As the blood builds up over months and years, it turns brown. When it ruptures, the material spills over into the pelvis and onto the surface of the uterus, bladder, bowel, and the corresponding spaces between. Treatment for endometriosis can be medical or surgical. Nonsteroidal anti-inflammatory drugs (NSAIDs) are frequently used first in patients with pelvic pain, particularly if the diagnosis of endometriosis has not been definitively established. The goal of directed medical treatment is to achieve an anovulatory state. Typically, this is achieved initially using hormonal contraception. This can also be accomplished with progestational agents (i.e., medroxyprogesterone), danazol, gestrinone, or gonadotropin-releasing hormone agonists (GnRH), as well as other less well-known agents. These agents are generally used if oral contraceptives and NSAIDs are ineffective. GnRH can be combined with estrogen and progestogen (add-back therapy) without loss of efficacy but with fewer hypoestrogenic symptoms. Laparoscopic surgical approaches include ablation of implants, lysis of adhesions, removal of endometriomas, uterosacral nerve ablation, and presacral neurectomy. They frequently require surgical removal. Conservative surgery can be performed to preserve fertility in young patients. Laparoscopic surgery provides pain relief and improved fertility over diagnostic laparoscopy without surgery. Definitive surgery is a hysterectomy and bilateral oophorectomy.
Pathological cysts
Other cysts are pathological, such as those found in polycystic ovary syndrome, or those associated with tumors.
A polycystic-appearing ovary is diagnosed based on its enlarged size — usually twice normal —with small cysts present around the outside of the ovary. It can be found in "normal" women, and in women with endocrine disorders. An ultrasound is used to view the ovary in diagnosing the condition. Polycystic-appearing ovary is different from the polycystic ovarian syndrome, which includes other symptoms in addition to the presence of ovarian cysts, and involves metabolic and cardiovascular risks linked to insulin resistance. These risks include increased glucose tolerance, type 2 diabetes, and high blood pressure. Polycystic ovarian syndrome is associated with infertility, abnormal bleeding, increased incidences of pregnancy loss, and pregnancy-related complications. Polycystic ovarian syndrome is extremely common, is thought to occur in 4-7% of women of reproductive age, and is associated with an increased risk for endometrial cancer. More tests than an ultrasound alone are required to diagnose polycystic ovarian syndrome.
Symptoms
Some or all of the following symptoms may be present, though it is possible not to experience any symptoms
»
Dull aching, or severe, sudden, and sharp pain or discomfort in the lower abdomen (one or both sides), pelvis, vagina, lower back, or thighs; pain may be constant or intermittent -- this is the most common symptom
»
Fullness, heaviness, pressure, swelling, or bloating in the abdomen
»
Breast tenderness
»
Pain during or shortly after beginning or end of menstrual period.
»
Irregular periods, or abnormal uterine bleeding or spotting
»
Change in frequency or ease of urination (such as inability to fully empty the bladder), or difficulty with bowel movements due to pressure on adjacent pelvic anatomy
»
Weight gain
»
Nausea or vomiting
»
Fatigue
»
Infertility
»
Increased level of hair growth
»
Increased facial hair or body hair
Menopause
The word menopause literally means the permanent physiological, or natural, cessation of menstrual cycles, from the Greek roots 'meno' (month) and 'pausis' (a pause, a cessation). In other words, menopause means the natural and permanent stopping of the monthly female reproductive cycles, and in humans this is usually indicated by a permanent absence of monthly periods or menstruation.
The word is commonly used in regard to human females, where menopause happens more or less in midlife, signaling the end of the fertile phase of a woman's life. Menopause is perhaps most easily understood as the opposite process to menarche.
Menopause in women cannot however simply be defined as the permanent "stopping of the monthly periods", because in reality what is happening to the uterus is quite secondary to the process. For medical reasons, the uterus is sometimes surgically removed (hysterectomy) in a younger woman, and after this her periods will cease permanently and the woman will technically be infertile, but as long as at least one of her ovaries still functions, the woman will not have entered menopause. This is because even without the uterus, ovulation, and the release of the sequence of reproductive hormones that are an essential part of the reproductive cycles, will continue until the time of menopause is reached.
Menopause is triggered by the faltering, shutting down, or surgical removal of the ovaries, which are a part of the body's endocrine system of hormone production, in this case the hormones which make reproduction possible and influence sexual behavior.
The process of the ovaries shutting down is a phenomenon which involves the entire cascade of a woman's reproductive functioning, from brain to skin, and this major physiological event usually has some effect on almost every aspect of a woman's body and life.
Overview
Menopause starts as the ovaries begin to fail to be able to produce an egg or ovum every month. Since the process of producing and ripening the egg is also what creates several of the key hormones involved in the monthly cycle, this in turn interrupts the regular pattern of the hormone cycles, and gradually leads to the somewhat chaotic and long-drawn out shutting down of the whole reproductive system.
The break-up in the pattern of the menstrual cycles not only causes the levels of most of the reproductive hormones to drop over time, but also causes the reproductive hormones to fall out of phase with one another, which often leads to extreme and unpredictable fluctuations in the levels, which itself can cause numerous symptoms in most women, such as hot flashes.
After a number of years of erratic functioning, the ovaries almost completely stop producing the estrogen hormones, and progesterone. Decrease in testosterone levels begins gradually in young adulthood, but testosterone levels are thought not to drop significantly during the menopause transition, because the stroma of the postmenopausal ovary, and the adrenal gland, still continue to secrete small amounts of testosterone even during post-menopause.
Because of the various hormonal changes, the reproductive system ceases to function.
Age of onset
The average age of menopause is 51 years. The normal age range for the occurrence of menopause is somewhere between the age of 45 and 55.
Last period ever occurring between the ages of 55 to 60 is known as a "late menopause". An "early menopause" on the other hand is defined as last period ever between the age of 40 to 45.
Rarely the ovaries stop working at a very early age, anywhere from the age of puberty to age 40, and this is known as premature ovarian failure (POF), also commonly referred to as "premature menopause" or "early menopause." 1% of women experience POF, and this is not considered to be due to the normal effects of aging. Some known causes of premature menopause include autoimmune disorders, thyroid disease, diabetes mellitus, chemotherapy, and radiotherapy, however, in the majority of spontaneous cases, the cause is unknown.
Premature menopause is diagnosed or confirmed by measuring the levels of follicle stimulating hormone (FSH) and luteinizing hormone (LH); the levels of these hormones will be abnormally high if menopause has occurred. Rates of premature menopause have been found to be significantly higher in fraternal and identical twins; approximately 5% of twins reach menopause before the age of 40. The reasons for this are not completely understood. Transplants of ovarian tissue between identical twins have been successful in restoring fertility.
Menopause in other species
Menopause in the animal kingdom appears perhaps to be somewhat rare, although this has not been thoroughly researched. However, it is already quite apparent that humans are not the only species that experience it. Menopause has been observed in rhesus monkeys[1], some cetaceans[2], as well as in a variety of other species of vertebrates including the guppy, the platyfish, budgerigars or “parakeets”, laboratory rats and mice, the opossum, and all manner of primates
Menopause in human evolution
The Grandmother hypothesis suggests that menopause evolved in humans because it promotes the survival of grandchildren. According to this hypothesis, post reproductive women feed and care for children, adult nursing daughters, and grandchildren whose mothers have weaned them. Human babies require large and steady supplies of glucose to feed the growing brain. In infants in the first year of life, the brain consumes 60% of all calories, so both babies and their mothers require a dependable food supply. Some evidence suggests that hunters contribute less than half the total food budget of most hunter-gatherer societies, and often much less than half, so that foraging grandmothers can contribute substantially to the survival of grandchildren at times when mothers and fathers are unable to gather enough food for all the children. In general, selection operates most powerfully during times of famine or other privation. So although grandmothers might not be necessary during good times, many grandchildren cannot survive without them during times of famine.
Infertility
Infertility primarily refers to the biological inability of a man or a woman to contribute to conception. Infertility may also refer to the state of a woman who is unable to carry a pregnancy to full term. There are many biological causes of infertility, some which may be bypassed with medical intervention.
Women who are fertile experience a natural period of fertility before and during ovulation, and they are naturally infertile during the rest of the menstrual cycle. Fertility awareness methods are used to discern when these changes occur by tracking changes in cervical mucus or basal body temperature.
Definition
There are strict definitions of infertility used by many doctors. However, there are also similar terms, e.g. subfertility for a more benign condition and fecundity for the natural improbability to conceive.
Infertility
Reproductive endocrinologists, the doctors specializing in infertility, consider a couple to be infertile if
the couple has not conceived after 12 months of contraceptive-free intercourse if the female is under the age of 34
the couple has not conceived after 6 months of contraceptive-free intercourse if the female is over the age of 35 (declining egg quality of females over the age of 35 account for the age-based discrepancy as when to seek medical intervention)
the female is incapable of carrying a pregnancy to term.
Subfertility
A couple that has tried unsuccessfully to have a child for a year or more is said to be subfertile. The couple's fecundability rate is approximately 3-5%. Many of its causes are the same as those of infertility. Such causes could be endometriosis, or polycystic ovarian syndrome.
Primary vs. secondary infertility
Couples with primary infertility have never been able to conceive,[2] while, on the other hand, secondary infertility is difficulty conceiving after already having conceived and carried a normal pregnancy. Technically, secondary infertility is not present if there has been a change of partners.
Some women are infertile because their ovaries do not mature and release eggs. In this case synthetic FSH by injection or Clomid (Clomiphene citrate) via a pill can be given to stimulate follicles to mature in the ovaries.
Prevalence
»
Generally, worldwide it is estimated that one in seven couples have problems conceiving, with the incidence similar in most countries independent of the level of the country's development.
»
Fertility problems affect one in seven couples in the UK. Most couples (about 84 out of every 100) who have regular sexual intercourse (that is, every 2 to 3 days) and who do not use contraception will get pregnant within a year. About 92 out of 100 couples who are trying to get pregnant do so within 2 years.
»
Women become less fertile as they get older. For women aged 35, about 94 out of every 100 who have regular unprotected sexual intercourse will get pregnant after 3 years of trying. For women aged 38, however, only 77 out of every 100 will do so. The effect of age upon men’s fertility is less clear.
»
In people going forward for IVF in the UK, roughly half of fertility prolems with a diagnosed cause are due to problems with the man, and about half due to problems with the woman. However about one in five cases of infertility have no clear diagnosed cause
»
In Britain, male factor infertility accounts for 25% of infertile couples, whilst 25% remain unexplained. 50% are female causes with 25% being due to anovulation and 25% tubal problems/other
»
In Sweden, approximately 10% of couples are infertile.[7] In approximately one third of these cases the man is the factor, in one third the woman is the factor and in the remaining third the infertility is a product of factors on both parts.
Causes
This section deals with unintentional causes of sterility. For more information about surgical techniques for preventing procreation, see sterilization.
Causes in either sex
For a woman to conceive, certain things have to happen: intercourse must take place around the time when an egg is released from your ovary; the systems that produce eggs and sperm have to be working at optimum levels; and your hormones must be balanced.
There are several possible reasons why it may not be happening naturally. In a third of cases, it can be because of male problems such as low sperm count.
Problems affecting women include endometriosis or damage to the fallopian tubes (which may have been ccaused by infections such as chlamydia).
Other factors that can affect your chances of conceiving including being over- or underweight or your age - female fertility declines sharply after the age of 35. Sometimes it can be a combination of factors, and sometimes a clear cause is never established.
Factors that can cause male as well as female infertility are
»
Genetic
◊
A Robertsonian translocation in either partner may cause recurrent spontaneous abortions or complete infertility.
A carcinoma is any malignant cancer that arises from epithelial cells. Carcinomas invade surrounding tissues and organs and may metastasize, or spread, to lymph nodes and other sites.
Carcinoma in situ (CIS) is a pre-malignant condition, in which some cytological signs of malignancy are present, but there is no histological evidence of invasion through the epithelial basement membrane.
Classification of carcinoma
Carcinoma, like all neoplasia, is classified by its histopathological appearance. Adenocarcinoma and squamous cell carcinoma, two common descriptive terms for tumors, reflect the fact that these cells may have glandular or squamous cell appearances respectively. Severely anaplastic tumors might be so undifferentiated that they do not have a distinct histological appearance (undifferentiated carcinoma).
Sometimes a tumour is referred to by the presumptive organ of the primary (eg carcinoma of the prostate) or the putative cell of origin (hepatocellular carcinoma, renal cell carcinoma).
Types of lung carcinoma
»
Adenocarcinoma is a malignant tumor originating in the epithelial cells of glandular tissue and forming glandular structures. This is common in the lung (forming 30-40% of all lung carcinomas). It is found peripherally, arising from goblet cells or type II pneumocytes.
»
Squamous cell carcinoma due to squamous metaplasia. This accounts for 20-30 percent of lung tumors and is usually hilar in origin.
»
Small cell carcinoma is almost certainly due to smoking. These metastasise early, and may secrete ADH (lowering patient sodium concentration).
»
Large cell undifferentiated carcinomas account for 10-15 percent of lung neoplasms. These are aggressive and difficult to recognise due to the undifferentiated nature. These are most commonly central in the lung.
»
Sinonasal undifferentiated carcinoma
Cervix
The cervix (from Latin "neck") is the lower, narrow portion of the uterus where it joins with the top end of the vagina. It is cylindrical or conical in shape and protrudes through the upper anterior vaginal wall. Approximately half its length is visible with appropriate medical equipment; the remainder lies above the vagina beyond view. It is occasionally called "cervix uteri", or "neck of the uterus".
Ectocervix
The portion projecting into the vagina is referred to as the portio vaginalis or ectocervix. On average, the ectocervix is 3 cm long and 2.5 cm wide. It has a convex, elliptical surface and is divided into anterior and posterior lips.
External os
The ectocervix's opening is called the external os. The size and shape of the external os and the ectocervix varies widely with age, hormonal state, and whether the woman has had a vaginal birth. In women who have not had a vaginal birth the external os appears as a small, circular opening. In women who have had a vaginal birth, the ectocervix appears bulkier and the external os appears wider, more slit-like and gaping.
Endocervical canal
The passageway between the external os and the uterine cavity is referred to as the endocervical canal. It varies widely in length and width, along with the cervix overall. Flattened anterior to posterior, the endocervical canal measures 7 to 8 mm at its widest in reproductive-aged women.
Internal os
The endocervical canal terminates at the internal os which is the opening of the cervix inside the uterine cavity.
Cervical crypts
There are pockets in the lining of the cervix known as cervical crypts. They function to produce cervical fluid.
Cervical mucus
Mucus plug
Cervical mucus
After a menstrual period ends, the external os is blocked by mucus that is thick and acidic. This "infertile" mucus blocks spermatozoa from entering the uterus.[5] For several days around the time of ovulation, "fertile" types of mucus are produced: they have a higher water content, are less acidic, and have a ferning pattern that helps guide spermatozoa through the cervix.[6] This ferning is a branching pattern seen in the mucus when observed with low magnification.
Some methods of fertility awareness involve estimating a woman's periods of fertility and infertility by observing changes in her body. Among these changes are several involving the quality of her cervical mucus: the sensation it causes at the vulva, its elasticity (spinnbarkeit), its transparency, and the presence of ferning.
Most methods of hormonal contraception work primarily by preventing ovulation, but their effectiveness is increased because they prevent the fertile types of cervical mucus from being produced. Conversely, methods of thinning the mucus may help to achieve pregnancy. One suggested method is to take guaifenesin in the few days before ovulation.
During pregnancy the cervix is blocked by a special antibacterial mucosal plug which prevents infection, somewhat similar to its state during the infertile portion of the menstrual cycle. The mucus plug comes out as the cervix dilates in labor or shortly before.
Cervical position
After menstruation and directly under the influence of estrogen, the cervix undergoes a series of changes in position and texture. During most of the menstrual cycle, the cervix remains firm, like the tip of the nose, and is positioned low and closed. However, as a woman approaches ovulation, the cervix becomes softer, and rises and opens in response to the high levels of estrogen present at ovulation.[1] These changes, accompanied by the production of fertile types of cervical mucus, support the survival and movement of sperm.
Functionality
During menstruation the cervix stretches open slightly to allow the endometrium to be shed. This stretching is believed to be part of the cramping pain that many women experience. Evidence for this is given by the fact that some women's cramps subside or disappear after their first vaginal birth because the cervical opening has widened.
During childbirth, contractions of the uterus will dilate the cervix up to 10 cm in diameter to allow the fetus to pass through.
During orgasm, the cervix convulses and the external os dilates. Dr. R. Robin Baker and Dr. Mark A. Bellis, both at the University of Manchester, first proposed that this behavior worked in such a way as to draw any semen in the vagina into the uterus, increasing the likelihood of conception. Later researchers, most notably Elisabeth A. Lloyd, have questioned the logic of this theory and the quality of the experimental data used to back it.
Cervical cancer
In humans the cervix may be affected by cervical cancer, a particular form of cancer which is detectable by cytological study of epithelial cells removed from the cervix in a process known as the pap smear. Evidence now shows that those with exposure to HPV (human papilloma virus) are at increased risk for cervical cancer. These viruses are related to the viruses that causes warts. The incidence of new cases of cervical cancer in the United States was observed to be 7 per 100,000 women in 2004.
Lymphatic drainage
The lymphatic drainage of the cervix is along the uterine arteries and cardinal ligaments to the parametrial, external iliac vein, internal iliac vein, and obturator and presacral lymph nodes. From these pelvic lymph nodes, drainage then proceeds to the paraaortic lymph nodes. In some women, the lymphatics drain directly to the paraaortic nodes.